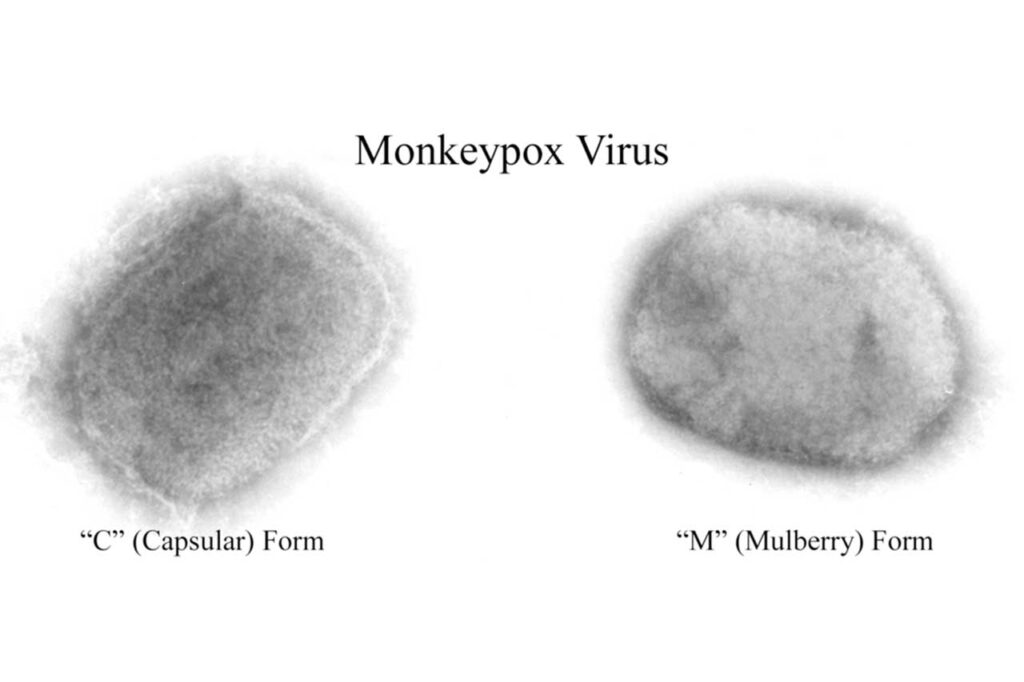
Congo to receive first mpox vaccines to address outbreak; The latest health stories from around the world
mpox declared public health emergency of international concern; The latest health stories from around the world